

The Rise of Intersectionality
Recently chemistry professor Dr. Maitland Jones Jr. was fired after 82 of his students signed a petition noting that his organic chemistry class was “too hard.” The students accused Jones of purposely making the class difficult, citing that their low scores negatively impacted their “well-being,” and their chances of getting into medical school. Instead of evaluating the rigor and substance of Jones’ curriculum, NYU justified its hasty action by noting the class’s unfavorable student reviews.
In response to the disciplinary action, former medical humanities professor and bioethicist Dr. Alice Dreger blasted the move in a tweet, saying it “made her skin crawl.”
“We aren’t going to end up with good doctors by letting undergrad pre-meds pass organic chem because universities want to protect their US News rankings,” she wrote.
The reaction is justified considering how standards for pre-med programs and even medical schools have shifted in the direction of equity and social justice. It seems that even professors cannot hold the line on academic performance, when the institutions they teach at make it a secondary importance to accommodating students’ sensitivities on the basis of how faulted or victimized they feel while learning in the highly competitive and demanding field of medicine.
The shift in a medicine-based education to an emphasis on race and social concern was highlighted by former University of Pennsylvania Medical School Dean Stanley Goldfarb, who stated:
“…Today a master’s degree in education is often what it takes to qualify for key administrative roles on medical-school faculties. The zeitgeist of sociology and social work have become the driving force in medical education. The goal of today’s educators is to produce legions of primary care physicians who engage in what is termed ‘population health.’”
Medical schools’ administrations seem to have become taken over by sociologists and critical race theorists—if not in title, then certainly in practice.
Most recently in the news, the University of Minnesota Medical School conducted a white coat ceremony for its Class of 2026, where each student had to recite a modified Hippocratic Oath which—on top of pledging to do no harm and to help the sick whenever possible—would “honor all Indigenous ways of healing that have been historically marginalized by Western medicine…white supremacy, colonialism, and the gender binary.”
The politicization of medicine has greater effects than just this sort of political white-knighting. Instead of focusing on promoting preventative care and treatment based on actual medical effectiveness, the impetus behind these medical schools’ actions seems to be entirely race-based. For example, Georgetown University is funding the study and formation of courses to prevent ‘microaggressions’ in medicine.
Likewise, the Association of American Medical Colleges released a new standard for teaching medicine which requires students to achieve ‘competencies’ in ‘white privilege’ or risk failing. It also seeks to do away with the ideas of gender and race, the latter of which the AAMC describes as “… a social construct that is a cause of health and health care inequities, not a risk factor for disease.” If this is the case, then how will doctors address the pervasiveness of Sickle-Cell Anemia and Multiple Myeloma in African-American communities, the prevalence of diabetes in Asian groups, or the largely unknown effects of hormonal therapies in minors?
THIS STRATEGY’S PRACTICAL CONSEQUENCES
This dramatic shift from upholding course standards to molding medicine in a racial lens is concerning. Though proponents of such measures would argue this is critical to improving race-relations in medicine and to deconstructing students’ “implicit biases,” saving lives and providing exceptional preventative care supersedes that.
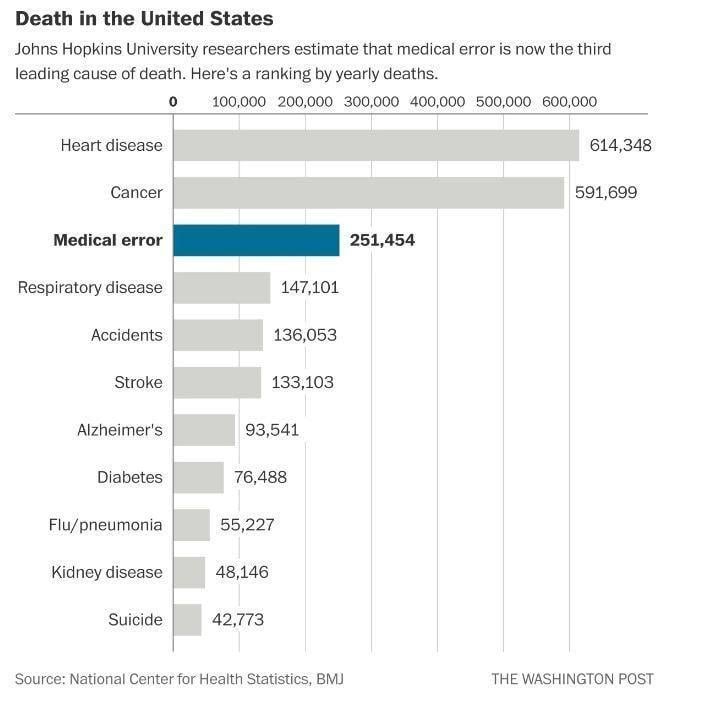
A 2016 BMJ analysis found that medical errors in health-care facilities are actually incredibly common and may even be the third-leading cause of death in the US. Medical malpractice accounts for about 251,000 deaths every year—this is more than accidents, stroke, Alzheimer’s, and respiratory disease:
A doctor’s most important duty to his or her patient is to do no harm—this includes preventing negligence, refraining from superfluous procedures, and ensuring every avenue of care is addressed prior to conducting invasive surgery. From shoddy hospital conditions to inexperienced nurses to just bad doctors, healthcare resulting in patient harm is a much more pressing issue than the alleged microaggressions resident doctors give off during their rotations.
The race and gender of a practicing physician should not matter as long as they are skilled, capable, and reasonable in their practice. It is therefore the universities and medical schools’ responsibility to uphold the rigorous standards they once had in order to ensure their students are prepared to work in high-stress, highly complicated medical scenarios—above all else. We need capable and skilled doctors.
No one ask about the race or gender of the surgeon when you are having brain surgery – ask Dr. Ben Carson Just like no one should care about your lawyers race or gender when you are in front of a jury – ask RBG and Johnnie Cochran. Might I add that no one should hire a professional because of their clown show tv commercials or billboards – it should be based on their merit and service. If we hire people based on factors beyond ability, then we do two things: stop the opportunity of those that have the ability and set up those without the ability for failure. Either way those being served will be impacted – we as attorneys call that negligence/malpractice.
According to the study above medical error is already a leading cause of death in the USA. Do we really want to exacerbate that concern by instead of having the most capable people trained, we focus on other factors for qualification? I know I want the most capable surgeon possible, just like when people hire Winslow Law to serve their legal needs it is due to our ability and service.
Recently, the ABA decided to end the LSAT requirement to enter law school, in order to eliminate a barrier for minorities to enter the legal field. If it really is a barrier then offer it for free to all people that qualify, but don’t lower the requirements to become an attorney. We need to remember that we serve our community and they deserve the best we can offer. Now we know why the reputation of the profession is deteriorating.
On the other hand, I am thankful for the work. Give us a call if you experience negligence or malpractice and let our experience, merit, and service speak for itself.